A woman’s hips are big, so it’s easy to have children?
Original Zhimei Tencent Medical Code, she knows

In daily life, I sometimes hear the saying that "a big ass is easy to bear."
This statement not only disrespects women, but also lacks scientific basis.

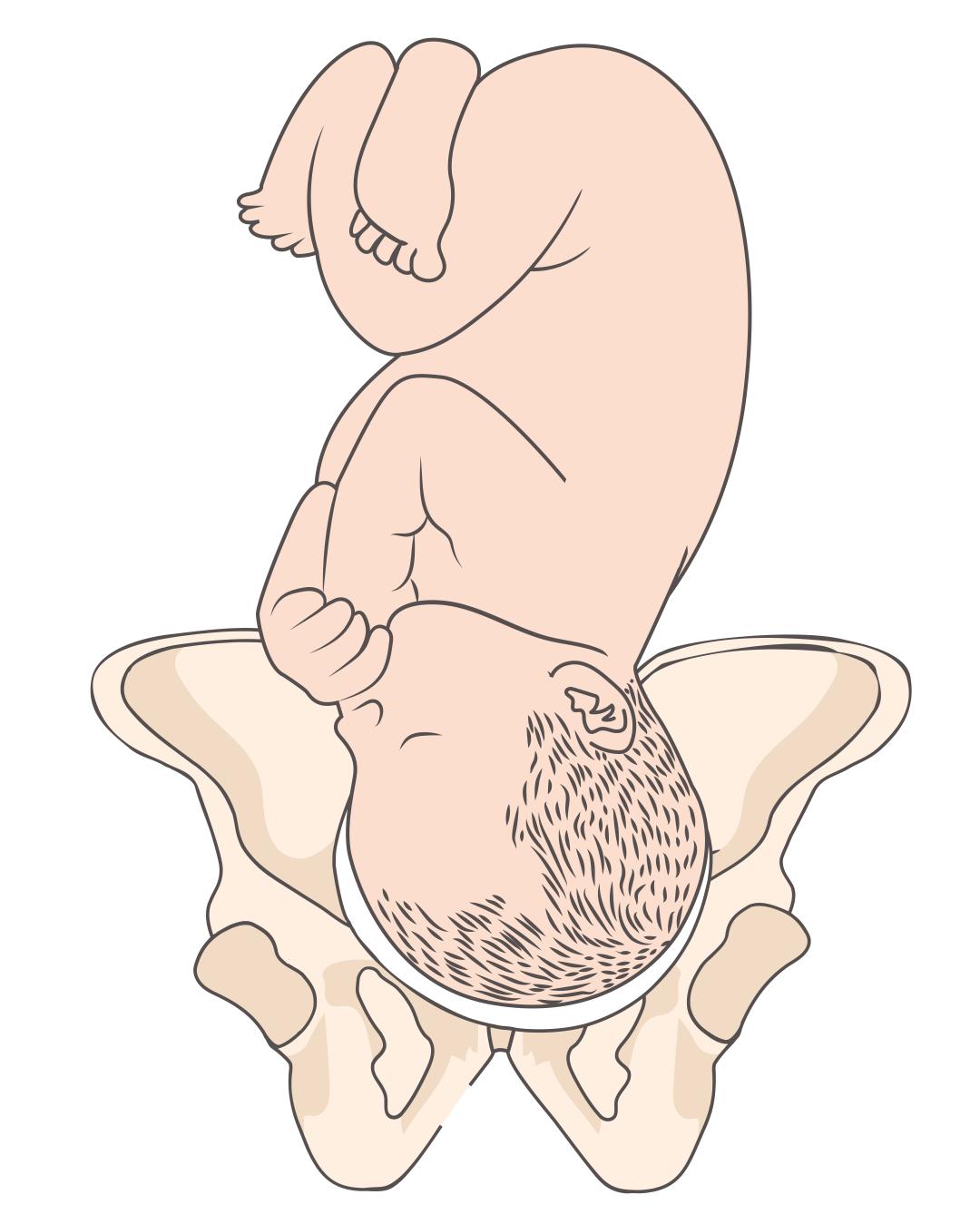
The so-called "good childbirth" usually means easy delivery, and one of the key factors affecting delivery is the size of the bone birth canal (the birth canal formed by the pelvic cavity).
During pregnancy, the size of the pelvis will not change much, but under the action of hormones such as relaxin, the ligament will relax and the pubic symphysis will be widened by 4-6 mm, so that the fetus can pass [1].
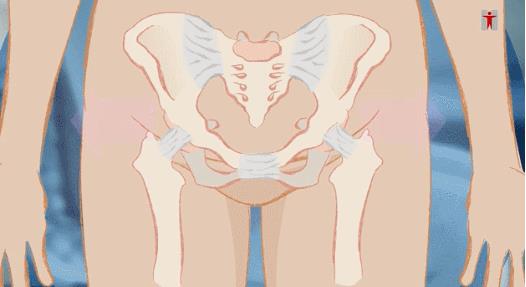
(Source: Hong Kong, China Department of Health)
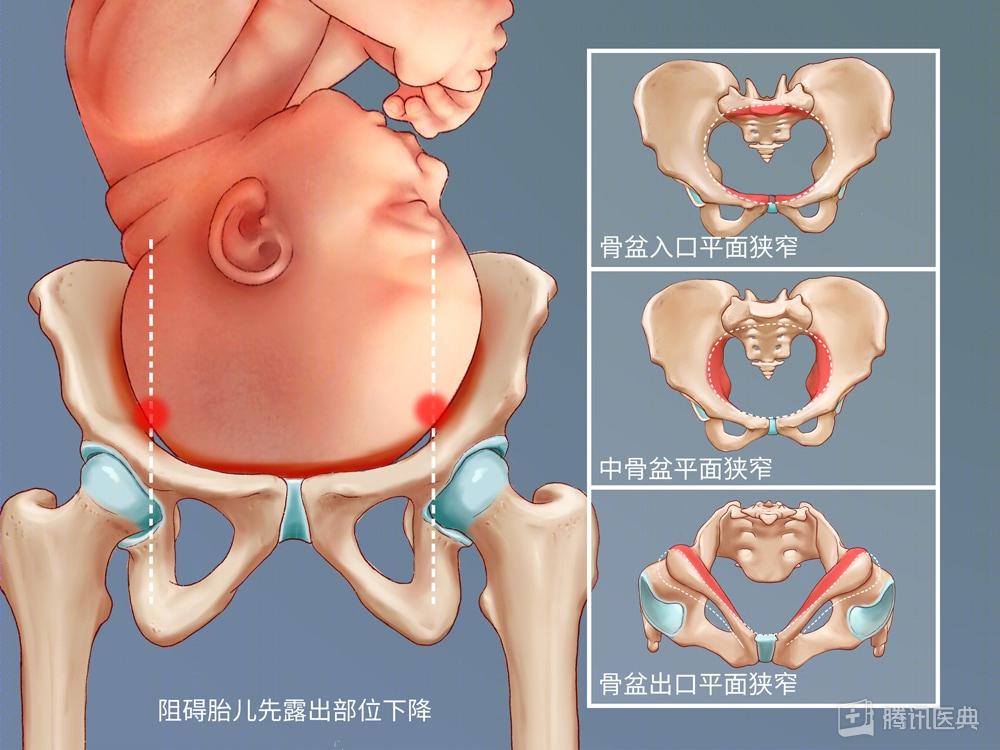
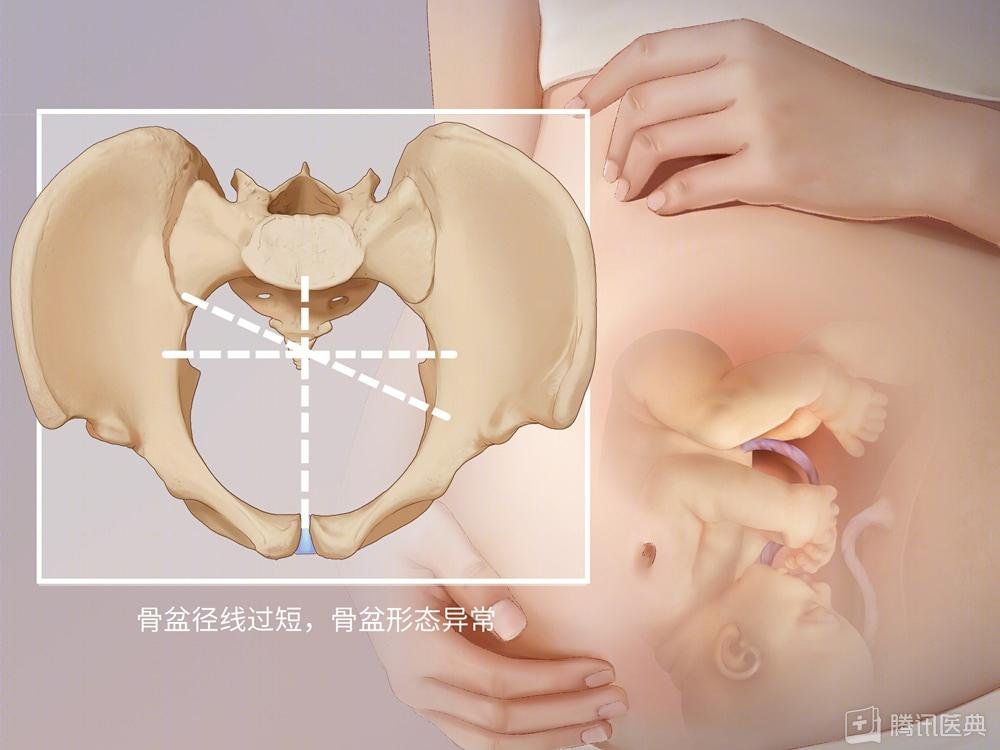
If the pelvis is too small, or the shape does not match the fetal head, it may affect the fetus passing through the pelvis and cause dystocia [1,2].
If the pelvis size is normal, but the fetus is too large, making the pelvis relatively narrow, it may also cause dystocia [1,2].
But a big ass doesn’t mean a big pelvis.
Under normal circumstances, the pelvic shape can’t be observed by naked eyes. Generally, a professional pelvic evaluation is conducted by a doctor during the prenatal examination.
The doctor will check and measure the size of the pelvic entrance, middle and exit, and then compare it with the size of the fetal head to see if there is pelvic stenosis or mismatch [1].

If the buttocks are fat, it will affect delivery.
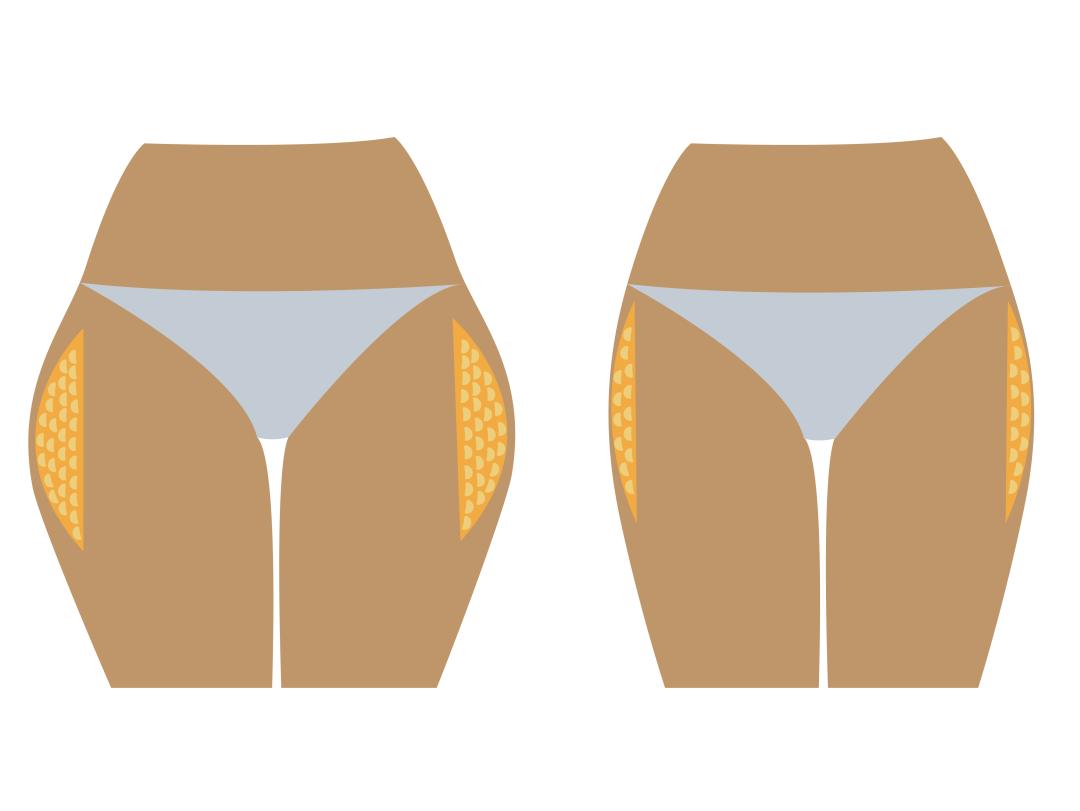
During pregnancy, estrogen and progesterone levels will continue to rise, causing an increase in fat reserves.
Especially in thighs, abdomen, buttocks, breasts and other parts of the fat increase is more obvious.
At this time, if the weight is not strictly controlled, too much fat will accumulate in the abdomen and buttocks, which will not only help the delivery, but also hinder the delivery process [3,4].
In addition, if the weight gain during pregnancy is too fast and too large, it is easy to cause the fetus to be larger and difficult to pass through the birth canal, resulting in dystocia [1-4].

1. Regular check-ups are more reassuring.
Delivery is a big project. Besides the pelvis, the productivity, the size and position of the fetus and the age of the pregnant woman will all affect delivery.
Therefore, regular check-ups during pregnancy can help doctors evaluate and make reasonable suggestions in time.
2. Don’t eat too much
Too fast weight gain during pregnancy will not only make the fetus too big, but also cause dystocia.
It will also increase the risks of gestational diabetes, pregnancy-induced hypertension and proteinuria.
It is also easy to separate rectus abdominis, and it is more difficult to return to normal weight after delivery [5,6].
Therefore, it is recommended that you consult a doctor or a clinical dietitian during the prenatal examination, and gain weight reasonably under the guidance of a doctor according to different body mass indexes before pregnancy.
3. Exercise is the most cost-effective "maintenance"
If pregnant women are healthy and have no pregnancy complications (such as threatened abortion, pre-eclampsia, cardiovascular diseases, placenta previa, etc.), 150 minutes of moderate and low-intensity aerobic exercise (such as walking and resistance training) per week is safe and has many benefits [7].
For example, it can control excessive weight gain, prevent gestational diabetes, enhance muscle strength, reduce low back pain and edema, improve the mood and sleep of pregnant women, and enhance their physical strength to prepare for production.
If there is no physical discomfort, it is recommended that pregnant women exercise at least five times a week for 30 minutes each time [8].
Sisters who have no exercise habits before can try low-intensity exercise, such as walking, brisk walking and cycling.
(Source: Hong Kong, China Department of Health)
If you have exercise habits at ordinary times, you can try moderate-intensity sports.
For example, jogging, aerobics, swimming, dancing, pilates, etc., and appropriately reduce the number after the number of weeks of pregnancy increases, according to the doctor’s advice.

Of course, strong abdominal muscles, pelvic floor muscles, etc. can not be practiced for a while, and the improvement of muscle strength depends on long-term persistence.
So sisters can exercise before they get pregnant and stick to it!
4. Encouragement from family and friends is especially important.
In addition to various objective conditions, there is also a great influence on natural delivery, that is, the mental and psychological state of the parturient.
Excessive anxiety, fear and tension may make pregnant women have uterine atony and prolong the labor process;
Fetal distress may also occur, which brings danger to the mother and baby [9,10].

Therefore, psychological construction during pregnancy is also crucial.
A good way to reduce fear is to understand the knowledge related to childbirth [11], such as hospital propaganda videos and brochures are good sources of knowledge.
Besides relying on the efforts of the parturient, encouragement and support from society, family, friends and medical staff are also very important [11,12], even more important.
Therefore, if your lover is pregnant, I hope you can learn more about it, understand her hardships, and give support and companionship.
Finally, there are many factors that affect delivery, and expectant mothers who are preparing for pregnancy really don’t have to worry about some accidental statement.
Regular check-ups, trusting doctors and nurses, and making adequate preparations will surely usher in that lovely baby happily!
Review expert
Feng Cuiping | Deputy Chief Physician, Department of Obstetrics and Gynecology, Beijing China-Japan Friendship Hospital
references
[1] Pavli?ev M, Romero R, Mitteroecker P. Evolution of the human pelvis and obstructed labor: new explanations of an old obstetrical dilemma. Am J Obstet Gynecol. 2020 Jan; 222(1):3-16. doi: 10.1016/j.ajog.2019.06.043. Epub 2019 Jun 25. PMID: 31251927.
[2]Nicholson JM, Kellar LC. The active management of impending cephalopelvic disproportion in nulliparous women at term: a case series. J Pregnancy. 2010; 2010:708615. doi:10.1155/2010/708615
[3] Siega-Riz AM, Viswanathan M, Moos MK, Deierlein A, Mumford S, Knaack J, et al. A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: birthweight, fetal growth, and postpartum weight retention. Am J Obstet Gynecol 2009; 201:339.e1–14.
[4]Kim SY, Sharma AJ, Sappenfield W, Wilson HG, Salihu HM. Association of maternal body mass index, excessive weight gain, and gestational diabetes mellitus with large-for-gestational-age births. Obstet Gynecol. 2014 Apr; 123(4):737-44. doi: 10.1097/AOG.0000000000000177. PMID: 24785599; PMCID: PMC4548850.
[5] Wang Linjie, Guo Honghua, Zhang Caihong, li miao, Zhu Jinmei, Yi Huanying, Chen Xiaomei. Research progress of weight management during pregnancy [J]. China Journal of Reproductive Health, 2019,30(03):284-287.
[6] Kominiarek MA, Peaceman AM. Gestational weight gain. Am J Obstet Gynecol. 2017; 217(6):642-651. doi:10.1016/j.ajog.2017.05.040
[7]Activity P , Pregnancy E D . Committee Opinion No. 650:, Physical Activity and Exercise During Pregnancy and the Postpartum Period[J]. Obstetrics & Gynecology, 2015, 126(6):e135.
[8] Professional Committee of Pregnancy Complicated with Diabetes Mellitus of China Maternal and Child Health Association, Obstetrics Group of Obstetrics and Gynecology Branch of Chinese Medical Association. Expert Consensus on Exercise during Pregnancy (Draft) [J]. Chinese Journal of Perinatal Medicine, 2021,24(09):641-645.
[9] Qian Shu Hua, Zhu Xinli, Shen Beibei, Zhou Huixin, Ding Yan. The influence of anxiety in early pregnancy and late pregnancy on maternal delivery mode [J]. Chinese Journal of Nursing, 2021,56(02):245-249.
[10] Rouhe H,Salmela-Aro K,Toivanen R,et al. Obstetric outcome after intervention for severe fear of childbirth in nulliparous women-randomised trial[J]. BJOG,2013,20:75-8
[11] Salmela-Aro K, Read S, Rouhe H, Halmesm?ki E, Toivanen RM, Tokola MI, Saisto T. Promoting positive motherhood among nulliparous pregnant women with an intense fear of childbirth: RCT intervention. J Health Psychol. 2012 May; 17(4):520-34. doi: 10.1177/1359105311421050. Epub 2011 Sep 29. PMID: 21963681.
[12] Clinical Practice Guidelines for Normal Delivery [J]. Chinese Journal of Perinatal Medicine, 2020,23(06):371-375.
Content production

Read the original text